Hodnocení prodloužení QT u dětí s cirhózou a její souvislost se závažností nemocí jater
Seyed Mohsen Dehghani1, Iraj Shahramian2, Masoud Tahani2, Maryam Ataollahi1, Nima Mehdizadegan1, Samaneh Zare1
+ Pracoviště
Souhrn
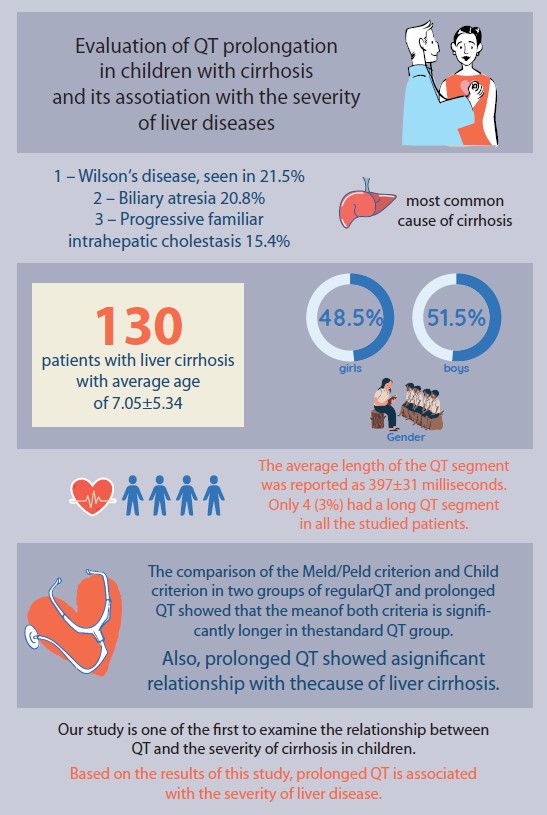
Úvod: Prodloužení QT intervalu na elektrokardiogramu (EKG) je pozorováno u více než 60 % dospělých s pokročilou cirhózou. Podle pečlivého výzkumu měli lidé s cirhózou, kteří mají prodloužené QT intervaly, horší míru přežití, závažnější příznaky onemocnění a rychlejší vývoj jejich stavu. Vzhledem k důležitosti predikce komplikací jaterní cirhózy u dětí a omezenému počtu studií týkajících se vztahu mezi prodlouženým QT a závažností jaterního onemocnění u dětí v této studii bylo zkoumáno prodloužené QT u dětí s jaterní cirhózou a její vztah k závažnosti jaterního onemocnění. Metody: V této studii byly děti do 18 let s jaterní cirhózou hodnoceny v seznamu transplantací jater odeslaných do nemocnice Abu Ali Sina Organ Transplantation Hospital v Shirazu v letech 2019 až 2021. QT bylo vypočteno na základě 12svodové EKG z operace transplantace jater. Výsledky: V této studii bylo hodnoceno 130 pacientů s jaterní cirhózou s průměrným věkem 7,05 ± 5,34. Průměrná délka QT segmentu byla hlášena jako 397 ± 31 milisekund. Pouze 4 (3 %) měli dlouhý QT segment u všech studovaných pacientů. Porovnání kritéria Meld/Peld a kritéria Child ve dvou skupinách s pravidelným QT a prodlouženým QT ukázalo, že průměr obou kritérií je významně delší ve skupině se standardním QT (p = 0,018; p = 0,038). Také prodloužené QT prokázalo významnou souvislost s příčinou jaterní cirhózy (p = 0,003). Závěr: Naše studie je jednou z prvních, která zkoumala vztah mezi QT a závažností cirhózy u dětí. Na základě výsledků této studie je prodloužený QT interval spojen se závažností onemocnění jater.
Klíčová slova
cirhóza, játra, děti, dlouhé QT, fibróza
Článek je v angličtině, prosím přepněte do originální verze.
Pro přístup k článku se, prosím, registrujte.
Výhody pro předplatitele
Výhody pro přihlášené
Literatura
1. Schuppan D, Afdhal NH. Liver cirrhosis. Lancet 2008; 371(9615): 838–851. doi: 10.1016/S0140-6736(08)60383-9.
2. Bircher J, Benhamou JP, McIntyre N et al. Oxford textbook of clinical hepatology. London: Oxford University Press 1999.
3. Sherlock S, Dooley J. Disease of the liver and biliary system. London: Blackwell 2002.
4. Schiff M, Sorrell MF, Maddrey WC. Schiff‘s disease of the liver. Philadelphia: Lippincott William & Wilkins 2003.
5. Schaffner F, Poper H. Capillarization of hepatic sinusoids in man. Gastroenterology 1963; 44(3): 239–242.
6. Djalalinia S, Tehrani FR, Afzali HM et al. Community mobilization for youth health promotion: A lesson learned from Iran. Iran J Public Health 2012; 41(4): 55–62.
7. Blachier M, Leleu H, Peck-Radosavljevic M et al. The burden of liver disease in Europe: a review of available epidemiological data. J Hepatol 2013; 58(3): 593–608. doi: 10.1016/ j.jhep.2012.12.005.
8. Anushiravani A, Sepanlou SG. Burden of liver diseases: a review from Iran. Middle East J Dig Dis 2019; 11(4): 189–191. doi: 10.15171/mej dd.2019.147.
9. Bucuvalas JC, Ryckman FC, Atherton H et al. Predictors of cost of liver transplantation in children: a single center study. J Pediatr 2001; 139(1): 66–74. doi: 10.1067/mpd.2001.115068.
10. Pinto RB, Schneider ACR, da Silveira TR. Cirrhosis in children and adolescents: An overview. World J Hepatol 2015; 7(3): 392–405. doi: 10.4254/wjh.v7.i3.392.
11. Santos JL, Choquette M, Bezerra JA. Cholestatic liver disease in children. Curr Gastroenterol Rep 2010; 12(1): 30–39. doi: 10.1007/s11894-009-0081-8.
12. Molleston JP, Sokol RJ, Karnsakul W et al. Evaluation of the child with suspected mitochondrial liver disease. J Pediatr Gastroenterol Nutr 2013; 57(3): 269–276. doi: 10.1097/MPG. 0b013e31829ef67a.
13. Shepherd RW. Chronic liver disease, cirrhosis, and complications: Part 1 (portal hypertension, ascites, spontaneous bacterial peritonitis (SBP), and hepatorenal syndrome (HRS)). Diseases of the Liver in Children: Springer 2014: 483–495. doi: 10.1007/978-1-4614-9005-0_25.
14. Högler W, Baumann U, Kelly D. Endocrine and bone metabolic complications in chronic liver disease and after liver transplantation in children. J Pediatr Gastroenterol Nutr 2012; 54(3): 313–321. doi: 10.1097/MPG.0b013e31823e9412.
15. Mircoli L, Rivera R, Bonforte G et al. Influence of left ventricular mass, uremia and hypertension on vagal tachycardic reserve. J Hypertens 2003; 21(8): 1547–1553. doi: 10.1097/00004872-2003 08000-00020.
16. Ruth ND, Drury NE, Bennett J et al. Cardiac and liver disease in children: Implications for management before and after liver transplantation. Liver Transplant 2020; 26(3): 437–449. doi: 10.1002/lt.25666.
17. Møller S, Henriksen J. Cardiovascular complications of cirrhosis. Postgrad Med J 2009; 85(999): 44–54. doi: 10.1136/gut.2006.112177.
18. Ruiz-del-Árbol L, Serradilla R. Cirrhotic cardiomyopathy. World J Gastroenterol 2015; 21(41): 11502–11521. doi: 10.3748/wjg.v21.41.11502.
19. Lantelme P, Khettab F, Custaud MA et al. Spontaneous baroreflex sensitivity: toward an ideal index of cardiovascular risk in hypertension? J Hypertens 2002; 20(5): 935–944. doi: 10.1097/00004872-200205000-00029.
20. Okada N, Takahashi N, Yufu K et al. Baroreflex sensitivity predicts cardiovascular events in patients with type 2 diabetes mellitus without structural heart disease. Circ J 2010; 74(7): 1379–1383. doi: 10.1253/circj.cj-09-0960.
21. Yufu K, Takahashi N, Okada N et al. Gender difference in baroreflex sensitivity to predict cardiac and cerebrovascular events in type 2 diabetic patients. Circ J 2011; 75(6): 1418–1423. doi: 10.1253/circj.cj-10-1122.
22. Fede G, Privitera G, Tomaselli T et al. Cardiovascular dysfunction in patients with liver cirrhosis. Ann Gastroenterol 2015; 28(1): 31–40.
23. Celtik C, Durmaz O, Oner N et al. Investigation of Cardiomyopathy in children with cirrhotic and noncirrhotic portal hypertension. J Pediatr Gastroenterol Nutr 2015; 60(2): 177–81. doi: 10.1097/MPG.0000000000000580.
24. Voiosu AM, Daha IC, Voiosu TA et al. Prevalence and impact on survival of hepatopulmonary syndrome and cirrhotic Cardiomyopathy in a cohort of cirrhotic patients. Liver Int 2015; 35(12): 2547–2555. doi: 10.1111/liv.12866.
25. Darstein F, König C, Hoppe‐Lotichius M et al. Preoperative left ventricular hypertrophy is associated with reduced patient survival after liver transplantation. Clin Transplant 2014; 28(2): 236–242. doi: 10.1111/ctr.12304.i.
26. Møller S, Henriksen J. Cirrhotic cardiomyopathy: a pathophysiological review of circulatory dysfunction in liver disease. Heart 2002; 87(1): 9–15. doi: 10.1136/heart.87.1.9.
27. Braverman AC, Steiner MA, Picus D et al. High-output congestive heart failure following transjugular intrahepatic portal-systemic shunting. Chest 1995; 107(5): 1467–1469. doi: 10.1378/chest.107.5.1467.
28. Milan A, Caserta MA, Del Colle S et al. Baroreflex sensitivity correlates with left ventricular morphology and diastolic function in essential hypertension. J Hypertens 2007; 25(8): 1655–1664. doi: 10.1097/HJH.0b013e3281ddb0a0.
29. Ates F, Topal E, Kosar F et al. The relationship of heart rate variability with severity and prognosis of cirrhosis. Dig Dis Sci 2006; 51(9): 1614–1618. doi: 10.1007/s10620-006-9073-9.
30. Puthumana L, Chaudhry V, Thuluvath PJ. Prolonged QTc interval and its relationship to autonomic cardiovascular reflexes in patients with cirrhosis. J Hepatol 2001; 35(6): 733–738. doi: 10.1016/s0168-8278(01)00217-3.
31. Dümcke CW, Møller S. Autonomic dysfunction in cirrhosis and portal hypertension. Scand J Clin Lab Invest. 2008; 68(6): 437–447. doi: 10.1080/00365510701813096.
32. Tentolouris N, Katsilambros N, Papazachos G et al. Corrected QT interval in relation to the severity of diabetic autonomic neuropathy. Eur J Clin Invest 1997; 27(12): 1049–1054. doi: 10.1046/j.1365-2362.1997.2300776.x.
33. Maser RE, Mitchell BD, Vinik AI et al. The association between cardiovascular autonomic neuropathy and mortality in individuals with diabetes: a meta-analysis. Diabetes care 2003; 26(6): 1895–1901. doi: 10.2337/diacare. 26.6.1895.
34. Voulgari C, Psallas M, Kokkinos A et al. The association between cardiac autonomic neuropathy with metabolic and other factors in subjects with type 1 and type 2 diabetes. J Diabetes Complications 2011; 25(3): 159–167. doi: 10.1016/j.jdiacomp.2010.06.001.
35. Bernardi M, Calandra S, Colantoni A et al. Q‐T interval prolongation in cirrhosis: prevalence, relationship with severity, and etiology of the disease and possible pathogenetic factors. Hepatology 1998; 27(1): 28–34. doi: 10.1002/hep.510270106.
36. Mohamed R, Forsey PR, Davies MK et al. Effect of liver transplantation on QT interval prolongation and autonomic dysfunction in end‐stage liver disease. Hepatology 1996; 23(5): 1128–1134. doi: 10.1002/hep.510230529.
37. Dillon J, Plevris J, Nolan J et al. Autonomic function in cirrhosis assessed by cardiovascular reflex tests and 24-hour heart rate variability. Am J Gastroenterol 1994; 89(9): 1544–1547.
38. Zhao J, Qi X, Hou F et al. Prevalence, risk factors and in- hospital outcomes of QTc interval prolongation in liver cirrhosis. Am J Med Sci 2016; 352(3): 285–295. doi: 10.1016/j.amjms.2016.06.012.
39. Bal JS, Thuluvath PJ. Prolongation of QTc interval: relationship with etiology and severity of liver disease, mortality and liver transplantation. Liver Int 2003; 23(4): 243–248. doi: 10.1034/j.1600-0676.2003.00833.x.
40. Liu H, Jayakumar S, Traboulsi M et al. Cirrhotic Cardiomyopathy: Implications for liver transplantation. Liver Transpl 2017; 23(6): 826–835. doi: 10.1002/lt.24768.
41. Fishberger SB, Rossi AF, Pittman NS. Prolongation of the QT interval in children with liver failure. Clinical cardiology 1999; 22(10): 658–660.
42. Ou M, Tian Y, Zhuang G et al. QTc interval prolongation in liver cirrhosis with upper gastrointestinal bleeding. Medicina Clínica (English ed.) 2021; 156(2): 68–75. doi: 10.1016/ j.medcli.2020.06.059.
43. Kim SM, George B, Alcivar-Franco D et al. QT prolongation is associated with increased mortality in end stage liver disease. World J Cardiology 2017; 9(4): 347–354. doi: 10.4330/wjc.v9.i4.347.
44. Mozos I, Costea C, Serban C et al. Factors associated with a prolonged QT interval in liver cirrhosis patients. J Electrocardiol 2011; 44(2): 105–108. doi: 10.1016/j.jelectrocard.2010.10.034.
45. Hajiani E, Masjedizadeh A, Ahmadi K. The prelevance of corrected qt interval in ECG and the severity of cirrhosis. J Res Med Sci 2003; 7: 319–321.
46. Héla E, Sofien K, Kamel L et al. QT interval abnormalities and heart rate variability in patients with cirrhosis. Arab J Gastroenterol 2020; 21(4): 246–252. doi: 10.1016/j.ajg.2020.08.001.
47. Hajiaghamohammadi AA, Daee MM, Zargar A et al. QT interval prolongation in cirrhosis: Relationship and severity. Caspian J Intern Med 2018; 9(3): 239–243. doi: 10.22088/cjim.9.3.239.
48. Tsiompanidis E, Siakavellas SI, Tentolouris A et al. Liver cirrhosis-effect on QT interval and cardiac autonomic nervous system activity. World J Gastroint Pathophysiol 2018; 9(1): 28–36. doi: 10.4291/wjgp.v9.i1.28.
49. Koshy AN, Ko J, Farouque O et al. Effect of QT interval prolongation on cardiac arrest following liver transplantation and derivation of a risk index. Am J Transpl 2021; 21(2): 593–603. doi: 10.1111/ajt.16145.
50. Biselli M, Gramenzi A, Lenzi B et al. Development and validation of a scoring system that includes corrected QT interval for risk analysis of patients with cirrhosis and gastrointestinal bleeding. Clin Gastroenterol Hepatol 2019; 17(7): 1388.e1–1397.e1. doi: 10.1016/ j.cgh.2018.12.006.